
WHAT IS PRESBYOPIA?
Presbyopia is an age-related inability to focus on close objects that results from either a loss of lens elasticity or a weakening of the ciliary muscles. With age, the eye’s ability to sharply focus on close objects gradually deteriorates.
Reading small print requires holding the book farther apart, which is a common symptom of presbyopia. Headaches and eyestrain may be related symptoms. The severity of problems will vary between individuals. Presbyopia may coexist with other types of refractive errors.
Mechanism and pathophysiology
- Age-related changes in the lens’ proteins. These changes cause the lenses to become harder and less elastic over time which leads to a decline in the accommodative power of crystalline lenses as people age.
- Age-related decline in ciliary muscle strength for accommodation or focusing.
Symptoms

- Blurred near vision even in good light.
- Eye strain,
- Headache, and
- Ocular discomfort
consequences of presbyopia:
It might seem like just another inconvenience that comes with getting older to many of us. However, untreated presbyopia can cause serious visual impairment, and over time, vision is likely to progressively deteriorate.
Additionally, untreated presbyopia, particularly in the geriatric population, has been a significant contributor to fall injuries and their co-morbidities. The co-morbidities, in addition to the vision loss brought on by untreated presbyopia, will make presbyopic patients more dependent on others, which will lower their quality of life.
Treatment / Management
Non-surgical Option
1. Spectacles:
Single vision lenses: Patients can comfortably read up close, but if they also have a refractive error for distance, they will need separate glasses for that as well.

BIFOCALS
There are two powers in this class of lenses. They offer correction for distance vision in the top half and near vision in the bottom half. The major disadvantage is the visible line between the top and bottom segments where the wearer notices image jump.
PROGRESSIVE LENSES
They are multifocal lenses, which means that in addition to correcting near and far vision, they also do so for intermediate vision, or the vision needed for arm’s-length activities like computer work.
When compared to bifocals, which have an image jump due to the separation of near and distance powers, progressive lenses seamlessly integrate these powers.
Those with complaints of brightness, haloes, discomfort, and blurred vision may need some time to adjust. But after 2 to 3 weeks of continued use, the symptoms usually go away.
2. Contact lenses:

Presbyopia can be managed in two ways with contact lenses.
- Monofocal contact lenses: A monofocal contact can correct near vision in one eye and distance vision in the other. Always correct for distance with the dominant eye. This idea is known as “monovision.” Monovision has the advantage of good vision at a wide range of distances, but it has the disadvantage of decreased contrast sensitivity and stereopsis.
- Multifocal contact lenses: There are various concentric zones on these lenses designed to correct distance, intermediate, and close vision.
3. PHARMACOLOGIC:

VUITY eye drops are the most popular in this category although other pharmacological drugs such as carbachol, brimonidine etc. are also being studied for the management of presbyopia. VUITY is 1.25% pilocarpine prescription eyedrop to help people with presbyopia primarily improve their ability to see up close by constricting their pupils.
This enhances accommodation and generates a pinhole effect, excluding dispersed light from the edges and allowing just the center parallel light rays to reach the eye. This gives a clear near image perception.
Surgical Options
Optically correcting presbyopia is common because it’s noninvasive, easy to do, and inexpensive.
With the help of bifocal glasses, multifocal progressive addition lenses, monofocal or bifocal contact lenses, presbyopes can achieve adequate distance and close-up vision without the risks of surgery.
However the emphasis now is on a method that is permanent and aesthetically pleasing , which is when surgical options become available.
The following techniques and procedures are among the most recent developments in the treatment of presbyopia:
1 Monovision laser ablation
2 Presbylasik
3 Presbyond
4 Lens extraction with lens implantation
5. Corneal inlays
Monovision LASIK:

The goal of this method is to eliminate or reduce the need for reading glasses using a laser corrective method.
Here, the dominant eye is corrected for distance while the non-dominant eye is made -1.5D myopic.
One drawback of monovision laser vision correction is that it frequently leads to decreased binocular visual acuity and depth perception (3D viewing).
Patients who have previously worn contact lenses for monovision typically adapt much more quickly.
PRESBYLASIK:
This is also a corneal procedure that uses a laser to reshape the cornea in a way that different zones can be used for viewing objects at different distances just like different refractive zones seen in multifocal lenses.
PRESBYOND:
Presbyond applies the Monovision principle. As a result, the non-dominant eye becomes myopic by -1.5D, while the dominant eye corrects for distance. Further, the extended depth of focus is achieved by generating a well-controlled spherical aberration.
With this procedure, patients should be able to view binocularly with clarity and have a good depth perception.
How can one tell which eye is dominant?
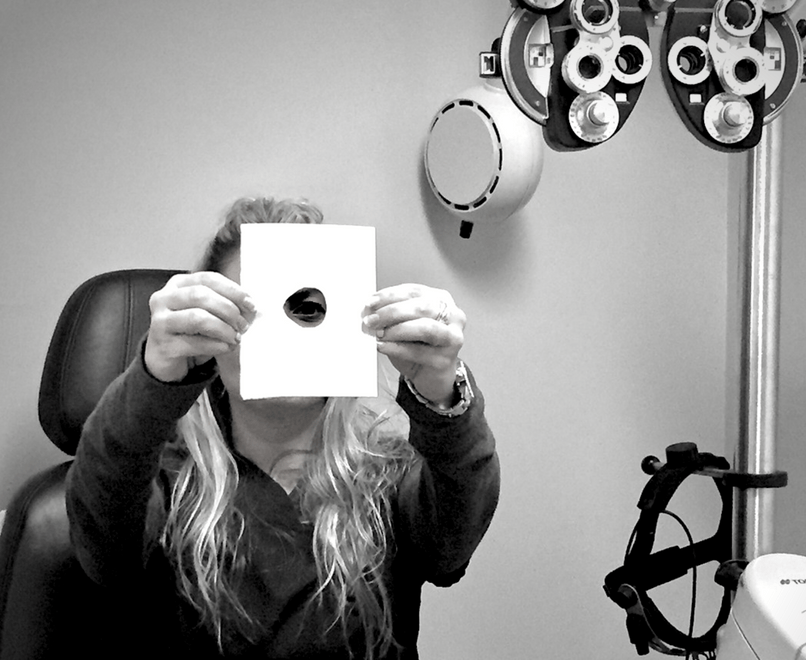
The Dolman technique is the simplest approach.
The hole-in-the-card test is another name for the Dolman method.
With both eyes open, the subject holds a card with a hole in the center and looks through the hole at a faraway object or Snellen 6/60 through the hole.
Next, the observer alternately closes their eyes. The dominant eye is the one that is looking through the hole at the object.
Lens extraction with IOL implantation:
The PRELEX (Presbyopic lens exchange) procedure involves replacing the natural crystalline lens (cataractous or pre cataractous) in the eye with an intra-ocular lens (IOL).
Using multifocal, trifocal, and extended depth of focus, this procedure can successfully minimize or reduce the need for reading glasses.
The majority of current multifocal IOL designs result in positive visual outcomes, with trifocal toric IOLs found to significantly outperform extended depth of focus IOLs in terms of near vision while producing comparable intermediate and distance VA results
1. Multifocal:
These lenses have multiple focal points for distance as well as near images.

Advantage:
- Reduces dependency on glasses for near and distance
Disadvantages:
- Requires glasses for intermediate distance
- Glare
- Halo around lights
- Difficult to do night driving
- Patients with retinal or optic nerve diseases are contraindicated
- Expensive when compared to monofocal IOLs
- Some may require glasses for fine near work, some distance work, working under dim illumination, or for fine-tuning the sharpness of images.
2. Trifocal:
These also have multiple focal points which cater to near, intermediate (computer/laptop work), and distance vision.
Advantage:
- Reduces dependency on glasses for near, intermediate, and distance vision.
Disadvantages:
- Expensive
- Patients with retinal or optic nerve diseases are contraindicated.
- Patients with unrealistic expectations of results, due to higher costs of surgery, are sometimes disappointed.
- just like with multifocal lenses, some patients with trifocal lenses may require glasses for fine near work, some distance work, working under dim illumination, or for fine-tuning the sharpness of images.
3. EDOF (Extended Depth Of Focus):
These lenses are designed to have a single focal point extended over a wide area covering all distances.

Advantages:
- Reduced dependency on near, intermediate, and distance vision glasses
- Minimal glare and halos around lights
- Better contrast sensitivity as compared to trifocals
- There is no total contraindication for patients with retinal or optic nerve diseases, and their doctors will be able to discuss their chances with them.
Disadvantages:
- May requires glasses to do fine near work like reading or threading
- Expensive
CORNEAL INLAYS
It is a corneal prosthetic inserted within the corneal layers of the non-dominant eye to reshape the cornea and improve refraction.
Most commonly used, FDA-approved corneal inlays are
- PRESBIA MICROLENS by Flexivue
This has a peripheral refractive power of +1.5D to +3.0D with central area having no refractive power.
- KAMRA by Acufocus
A central hole is present in this opaque disc. The central hole creates a pinhole effect and offers sharp central vision.
- RAINDROP by Revision
This entails inserting a hydrogel lenticule that will increase corneal curvature inside the cornea. Good near vision is achieved by this corneal reshaping.
CONCLUSION:
With the world’s population getting older, presbyopia is becoming more prevalent. An uncorrected case of presbyopia could significantly affect a patient’s quality of life and daily activities. The aim of this blog is to inform the readers about the range of available therapeutic modalities. Presbyopia awareness campaigns, counselling, appropriate optical corrections, and updates on recent developments in presbyopia management are the responsibility of eye care professionals.