
Studies have demonstrated that atropine eye drops can be used safely and effectively to control myopia. Let’s first examine what myopia progression is and why controlling it is important.
WHAT CAUSES REFRACTIVE ERROR
The main factor influencing refractive error is genetics. Research has shown that environmental factors like increased near work (reading, writing, etc.) can cause short or nearsightedness along with genetic predilection.
The factors that influence refraction in the eyes that don’t allow the light to focus on the retina properly are:
1. Size of the eyes (long or small)
2. The shape of the structure of the eye like cornea or lens (irregular/asymmetric/flat/steep)
The changes in size, shape, and aging lens cause different types of refractive error. Namely, Myopia, hypermetropia, astigmatism, and presbyopia.
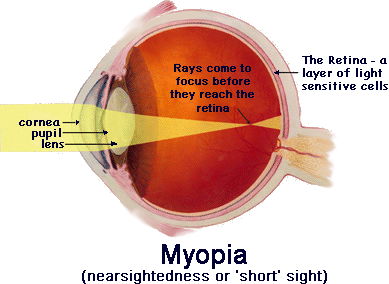
WHAT IS MYOPIA?
A person with nearsightedness, also known as myopia, has difficulty seeing things far away while being able to see nearby.
Myopia is usually seen in eyes that are too long or have strong focusing power. Therefore the image is formed in front of the retina.
MYOPIA IN CHILDREN
Humans are born far-sighted or hyperopes (+ number). Refraction of lesser than +0.75D at an early age is a strong predictor of future myopia.
Children under the age of 8 are most likely to develop myopia if they have the following risk factors:
- Refraction less than +0.75D (towards minus side) before the age of 8 years.
- Parental myopia: Having one parent who is myopic increases risk by 3 times and having both parents who are myopic increases risk by 6 times. The child is more likely to develop myopia if his or her sibling has it.
- CLEERE study shows that more near work and lesser outdoor activities can lead to near sightedness. According to THE AMERICAN ACADEMY OF PEDIATRICS:
- There should be no digital media use (except video-chatting) in children younger than 18 to 24 months.
- For children 18 months to 5 years, the AAP now recommends aiming for not more than one hour of screen entertainment per day and focusing on educational media. This is a cumulative period and should be divided throughout the day.
Read this to know about the harmful effects of unlimited screen time.
- Axial length: this is the distance between the anterior and posterior poles of the eye. The axial length in people with normal refraction grows about 0.1 mm per year between 6 and 9 years of age. Later, this decreases and stabilizes in late adolescence.
- According to CLEERE the axial length in future myopia patients grew by 0.33mm in the year before their myopia onset, and by 0.20mm or more per year after their myopia onset.
- Ethnicity: The progression of myopia is higher in East and Southeast Asian children than in any other race.
WHY IS IT IMPORTANT TO STOP THE PROGRESSION OF MYOPIA?
Myopia is a major public health issue and is the 6th leading cause of visual loss.
An increased minus number and a significant increase in axial length of the eye can increase the risk of cataracts, glaucoma, retinal detachment, and myopic maculopathy in patients.
MYOPIA PROGRESSION IN CHILDREN?
It is not clear when myopia stops progressing. The COMET (Correction Of Myopia Evaluation Trial) study suggested that the peak myopia deceleration of progression occurred at around 12 years.
The typical progression that occurs:
| AGE | TYPICAL PROGRESSION |
| <9 YEARS | -1D |
| 9-11 YEARS | -0.75D |
| 12-16 YEARS | -0.5D |
COMET found that:
- 48% had stable myopia by age 15 years;
- 77% by age 18 years;
- 90% by age 21 years;
- 96% of participants had stable myopia by 24 years of age.
In short, the majority of myopia stabilizes by the early-to-mid-20s, but around 20% of young myopes will still progress by at least 1D during those years
ATROPINE AND MYOPIA PROGRESSION
Atropine is anticholinergic which means it reduces secretions in the body, and relieves constriction and spasms. As a result of atropine, the pupil dilates and the eye is unable to accommodate, causing glare and blurred vision.
According to ATOM 1 (Atropine for the Treatment Of Childhood Myopia 1), Atropine 1% was effective in the treatment of childhood myopia, but it caused glare, blurred vision due to pupil dilation, and failure of accommodation, which resulted in using bifocals.
The ATOM 2 (Atropine for the Treatment Of childhood Myopia) study studied the safety and efficacy of lower doses of atropine, 0.5%, 0.1% and 0.01% doses.
The study shows that 0.01 % atropine taken every evening in each eye has very little effect on pupil dilation or accommodation and is effective for controlling myopia, although not as much as higher concentration, 1% in ATOM 1 study.
In addition, myopic rebound after cessation of drops was studied which showed that lower concentrations had a smaller effect in terms of myopic rebound than higher concentrations. ATOM 2 suggested 0.01% atropine as the best long-term solution for myopia progression with the least amount of symptoms.
In ATOM 2 there was no control group, and the effect of atropine on axial length was unclear, so the researchers conducted the 2 year LAMP STUDY: low concentration study for myopia progression. The results showed that there is no effect on axial length with 0.01% atropine, while 0.05% concentration is twice as effective at controlling myopia and axial length with the least side effects over 2 years. Therefore some doctors prescribe 0.05% atropine for myopia control.
HOW TO USE ATROPINE?
When progression is detected, the doctor typically prescribes low dose atropine in each eye every evening. A typical course of treatment lasts for about 3-5 years, depending on the outcome
There can be a rebound on stopping a higher concentration of atropine. The rebound is least with 0.01%. After cessation, the doctor may advise the individual to wear contact lenses or Ortho-K lenses.
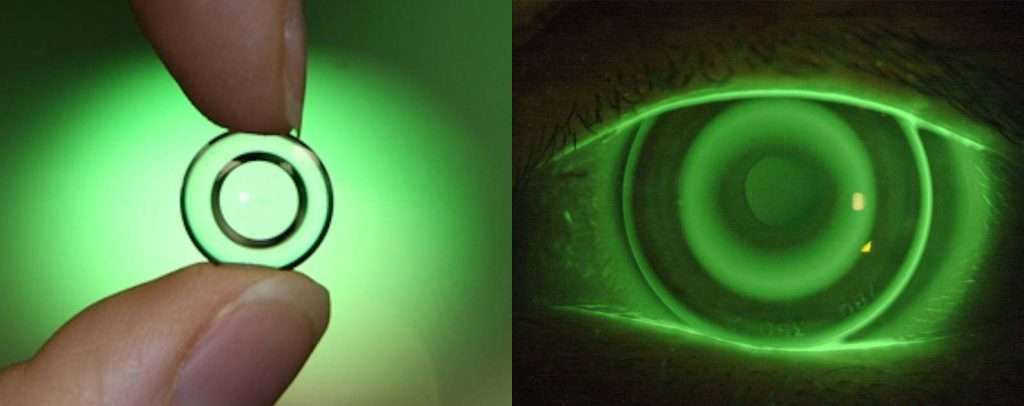
Ortho-K are customized gas permeable contact lenses that are worn at night (while sleeping) and removed in the morning. This reshapes the eye surface, improving vision the next day. Using Ortho-K lenses regularly can also slow myopia progression.
CONCLUSION
The management of myopia does not end once the doctor controls its progression. Routine eye examinations are imperative to monitor eye diseases that patients with high numbers (>-5D) or with axial lengths longer than 26mm are prone to. Among them are cataracts, glaucoma, retinal detachments, and myopic macular degeneration.